
Diffuse Axonal Injury in Traumatic Brain Injury
According to a study published in the New England Journal of Medicine on Christmas Day 2014, by David Wright, M.D. et al (Emory University) , more than 2.4 million ER visits, hospitalizations and deaths are attributable to Traumatic Brain Injury (TBI) annually in the United States, with 5.3 million individuals suffering from the after effects of TBI at any given time. TBI is responsible 12% of hospitalizations, and 76 billion dollars in total costs to American society every year, and afflicted individuals typically require 5-10 years of intensive therapy, often with very mixed results.
Traumatic Brain Injury
Traumatic brain injury (TBI), also called acquired brain injury or simply head injury, occurs when a sudden trauma causes damage to the brain. The damage can be focal (confined to one area of the brain) or diffuse (involving more than one area of the brain).
Concussion is the most common type of TBI. Technically, a concussion is a short loss of consciousness in response to a head injury, but in common language the term has come to mean any minor injury to the head or brain. Typically, there are no long term after effects on overall brain function from such injuries, but repeated concussions may result in long-term alterations in higher brain functions .
To date, no effective drug therapy has been found to improve outcomes in TBI. However, in recent years, promising studies conducted in animals with TBI have indicated significant improvements in cerebral edema, neuron loss and behavior deficits after early administration of of the neurosteroid progesterone. In addition, 2 relatively small single center clinical trials in humans seemed to indicate similar benefits with progresterone. Dr. Wright and his team set out to do a much larger multi-center trial to see if these promising results could be duplicated. Unfortunately, Dr. Wright’s study results did not show a statistically significant improvement in outcomes for patients given progesterone early in the course of TBI. For now anyway, the search for an effective pharmacologic treament for TBI goes on.
Definition of Diffuse Axonal Injury in TBI
Diffuse Axonal Injury is a potentially severe form of TBI, and is the underlying cause of injury in 50% of TBI patients requiring hospitalization. Diffuse Axonal Injury results from sudden changes in velocity of the head. Motor vehicle accidents (MVAs) are a frequent example of such situations. Severe TBI seen in MVAs arise as a result of acceleration-deceleration events of the brain within the skull, without skull fracture (so-called “closed head” trauma). This event usually occurs as vehicle occupants are thrown forward or sideways, resulting in collisions between the head and windshields, dashboards, etc. While the majority of severe brain injuries in acceleration-deceleration events result from DAI, other forms of traumatic brain injury such as contusion (bruising of tissues), anoxia (loss of oxygen flow to tissues), intracerebral hemorrhage, and penetrating cerebral trauma may occur at the same time, complicating cognitive deficits and prognosis. While many such injuries involve physical impact of the head with some portion of the vehicle, it is the sudden acceleration-deceleration of the head, apart from impact, that results in diffuse axonal injury. Some degree of diffuse axonal injury is considered to be present in any individual involved in an MVA who is rendered unconscious by head injury.
Many researchers now believe that long-term neurological deficits in football players, hockey players, and soccer players who have received multiple concussions is more closely related to diffuse axonal injury, rather than the concussive effects suffered on collision, as the symptom complex and course seen in these individuals is similar to patients involved in MVAs.
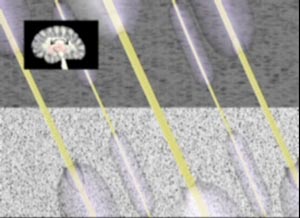
Diffuse Axonal Injury Mechanism
Diffuse Axonal Injury involves massive loss of neuronal function towards the central area of the brain, well away from any areas of direct trauma with the skull. Researchers were initially puzzled as to why such extensive damage occurred without direct trauma. The mechanism of DAI was subsequently discovered to occur as a result of rotational movement of the brain during acceleration-deceleration events. The key to understanding the injury lies in the varying densities of brain tissue. Grey matter (primarily the cerebral hemispheres) is less dense than white matter (i.e.- the brainstem and central brain structures). Due to different inertial characteristics based on these densities, as the brain rotates during acceleration-deceleration events, lower density tissues move more rapidly than those of greater density. This velocity difference causes shearing of neuronal axons which traverse the junction of gray and white matter, and explains why DAI lesions are seen most frequently in the areas of the brain where white and gray matter meet (see specific affected areas below). The term “shear injury” may be used interchangeably with DAI. The magnitude of axonal injury in DIA is dependent on 3 factors: 1) the distance from the center of rotation, 2) the arc of the rotation, and 3) the duration and intensity of the force.
Typically, the process is widespread and bilateral, most frequently involving the frontal and temporal lobe white matter, corpus callosum (bridge between the cerebral hemispheres), and areas of the brainstem not involved with basic life functions (cardiac and respiratory). As a result, individuals suffering from DAI rarely die. There is almost no correlation between DAI and the presence or absence of skull fractures, or subarachnoid or subdural bleeding.
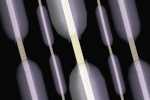
There appears to be two phases to the axonal injury in DAI. Primary injury, in which axons undergoing shear forces are stretched at the moment of impact, and then a secondary, or delayed phase, where stretched axons undergo swelling and rupture as a result of biochemical changes related to the primary injury. Initial abnormal changes in stretched axons, known as “bulb” formation, is generally seen within a day or two of injury, but completion of the degenerative process may take up to 2 years. While there is no hard clinical data correlating the neuronal degeneration to cognitive deficits, it is presumed that clinical symptoms may also take 2 years to fully develop in individuals who are not rendered unconscious at the time of initial injury. While mechanical separation of neuronal axons may occur at the moment of injury, it is now widely held that the greatest injury to neurons with DAI occurs as a result of primary strain (not rupture), followed by delayed secondary rupture due to metabolic disturbances within the neuronal axon, rather than tearing of axons at injury. Jay Meythaler, M.D. et. al. give a beautiful and detailed description of this process in their very in-depth review of DAI in a 2001 article in The Archives of Physical Medicine and Rehabilitation. In a paper published March 1st, 2013 in the Journal of Neurotrauma , Douglas Smith, M.D., et. al. also describe the pathological process of axonal injury in detail. In this paper, Dr Smith describes the formation of “axonal bulbs” – swellings at the ends of axons that eventually result in disconnection, as well as a process known as “beading” in which swellings, or “axonal varicosities”, occur along the length of a single axon, resulting in multiple points of interruption to neurotransmitter flow.
Diffuse Axonal Injury – Brain Areas Affected
The gray-white matter interface of the brain, where damage due to Diffuse Axonal Injury most frequently occurs, consists of tens of millions of neurons interconnecting all of the various distinct functional areas of the brain – it’s like a highly sophisticated communications complex. DAI results in disruption of these interconnecting neurons and has a devastating effect on overall neurological function.
Typically, the process is widespread and bilateral, most frequently involving the frontal and temporal lobe white matter, corpus callosum (bridge between the cerebral hemispheres), and areas of the brainstem not involved with basic life functions (cardiac and respiratory).
Diffuse Axonal Injury Effects on Neurological Function
The Adams classification categorizes DAI based on the degree and location of injury-related lesions in the white matter. In this classification, mild (grade 1) is characterized by microscopic changes in the white matter of the cerebral cortex, corpus callosum, brainstem, and occasionally the cerebellum. Moderate DAI (grade 2) is defined by grossly evident focal lesions isolated to the corpus callosum. In severe DAI (grade 3), there are additional focal lesions in the dorsolateral quadrants of the rostral brainstem (commonly in the superior cerebellar peduncle).
Severe DAI results in an immediate loss of consciousness, and most individuals with a severe DAI injury (>90%) remain in a persistent vegetative state. Essential cardiac and respiratory brain functions required for life are typically not affected by DAI, as these functions are located deep in the brainstem, away from the gray-white matter interface. As a result, DAI rarely causes death. The prognosis worsens in direct relationship to the number of lesions present.
The Glasgow Coma Scale, developed in 1974 by Jennett and Teasdale, is used by many clinicians as an initial assessment of neurological function in head injury patients. It involves scoring neurological function by assigning points for eye, verbal and motor functions, with the highest possible score of 15 being completely normal, and the lowest possible score of 3 consistent with coma or death. It is considered by many to be the best means of predicting long-term outcomes in patients affected by diffuse axonal injury (superior to findings on CT or MRI). In general, pateints with a GCS score of 8 or less immediately after injury have a poor prognosis for complete recovery.
Slightly less than 10% of individuals with severe DAI will regain consciousness. Improvement in neurological function in these individuals, if any, will usually occur within the first twelve months after injury. After this point, further resolution of deficits will be minimal to absent. Because DAI can affect virtually every higher brain function, deficits can consist of a broad range of cognitive problems.
Cognition is a term used to describe the processes of thinking, reasoning, problem solving, information processing, and memory. Most patients with severe DAI, if they recover consciousness, suffer from cognitive disabilities, including the loss of many higher-level mental skills. The most common cognitive impairment among severely head-injured patients is memory loss, characterized by some loss of specific memories and the partial inability to form or store new ones. Some of these patients may experience post-traumatic amnesia (PTA), either anterograde or retrograde. Anterograde PTA is impaired memory of events that happened after the DAI, while retrograde PTA is impaired memory of events that happened before the DAI.
Simon Fleminger, M.D., in an article in the Psychiatric Times in 2010, stated that measurement of PTA can provide a useful guide to prognosis in patients with Diffuse Axonal Injury. “As a rule, if PTA lasts less than 1 week, a reasonably good outcome is expected. If PTA lasts longer than 1 month, significant disability is likely; a good proportion of those affected will not be able to return to work or to independent living.In general, younger individuals (those in their late teens or 20s) tend to do much better.
Many patients with mild to moderate head injuries who experience cognitive deficits become easily confused or distracted and have problems with concentration and attention. They also have problems with higher level, so-called executive functions, such as planning, organizing, abstract reasoning, problem solving, and making judgments, which may make it difficult to resume pre-injury work-related activities. Many DAI patients have sensory problems, especially problems with vision. Patients may not be able to register what they are seeing or may be slow to recognize objects. Also, DAI patients often have difficulty with hand-eye coordination. Because of this, DAI patients may be prone to bumping into or dropping objects, or may seem generally unsteady. DAI patients may have difficulty driving a car, working complex machinery, or playing sports. Other sensory deficits may include problems with hearing, smell, taste, or touch.
Speech is often slow, slurred, and garbled. Some may have problems with intonation or inflection, called prosodic dysfunction. An important aspect of speech, inflection conveys emotional meaning and is necessary for certain aspects of language, such as irony. Affected individuals may lose a previous ability to speak a foreign language. These language deficits can lead to miscommunication, confusion, and frustration for the patient as well as those interacting with him or her.
Most DAI patients have emotional or behavioral problems that fit under the broad category of psychiatric health. Family members of DAI patients often find that personality changes and behavioral problems are the most difficult disabilities to handle. Psychiatric problems that may surface include depression, apathy, anxiety, irritability, anger, paranoia, confusion, frustration, agitation, insomnia or other sleep problems, and mood swings.
Problem behaviors may include aggression and violence, impulsivity, disinhibition, “acting out”, noncompliance, social inappropriateness, emotional outbursts, childish behavior, impaired self-control, impaired self-awareness, inability to take responsibility or accept criticism, egocentrism, inappropriate sexual activity, and alcohol or drug abuse/addiction. Some patients’ personality problems may be so severe that they are diagnosed with borderline personality disorder, a psychiatric condition characterized by many of the problems mentioned above. Sometimes DAI patients suffer from developmental stagnation, meaning that they fail to mature emotionally, socially, or psychologically after the trauma. This is a serious problem for children and young adults who suffer from a DAI. Attitudes and behaviors that are appropriate for a child or teenager become inappropriate in adulthood. Many DAI patients who show psychiatric or behavioral problems can be helped with medication and psychotherapy.
Diagnosis of Diffuse Axonal Injury
Virtually all individuals who are rendered unconscious by a closed head acceleration-deceleration event will suffer some degree of Diffuse Axonal Injury. While the mechanism of injury, and neuro-pychiatric and imaging study findings post-injury, may be highly suggestive of DAI, as of this writing, the definitive diagnosis of DAI can only be made post-mortem by a microscopic examination of brain tissue.
Imaging Studies in Diffuse Axonal Injury
Computed Tomography

Neither plain film xray, nor CT (Computed Tomography) can detect the actual damage to white matter tracts that is the essential finding in Diffuse Axonal Injury. Rather, findings on CT are related to small hemorrhages that occur in blood vessels which are stretched in close proximity to the injured nerve axons. These hemorrhages show up as punctate lesions, and are considered the “smoking gun” of Diffuse Axonal Injury. As you’ll see in this image, the findings appear very minimal for such a devastating injury. It’s important to note that CT findings of punctate lesions after head injury indicate that Diffuse Axonal Injury has occurred, and do not necessarily provide an accurate assessment of the extent of brain injury. The sensitivity of CT in detecting the full extent of DAI may be low, particularly in the early post-injury period. There may also be a very poor correlation between findings on imaging studies and actual neurological deficits. In the first several weeks post-injury, deficits tend to be greater than lesions on imaging studies would suggest, whereas at 12 months, the relationship is often inverted. Imaging one to two years out may show extensive brain atrophy in individuals whose deficits have actually improved due to re-assignment of brain functions from damaged to healthy areas.
Magnetic Resonance Imaging
Recently, a new MRI contrast imaging technique, Diffusion Tensor Imaging, holds the promise of more accurate and early assessment of injury to white matter nerve tracts within the brain. The technique is based on the proven observation that the diffusion of water through brain tissues is affected by changes in neuron axon structure at the microscopic level (as occurs in Diffuse Axonal Injury). While DTI appears to be very sensitive in detecting abnormalities in axon micro-architecture, interpretation of the scans as currently understood lacks specificity, making it difficult to assign a particular diagnosis from the spectrum of neurological diseases that may result in damage to white matter nerve tracts (ie – DAI, tumor, multiple sclerosis, stroke). Here is a fairly technical but nevertheless fascinating review of Diffusion Tensor Imaging from the National Institutes of Health.
More recently, an MRI modality known as MRI-DTI has shown great promise in detecting injury due to neuronal shear (as occurs in DAI). Joseph Wu, M.D., a neuroradiologist affiliated with U.C. Irvine, has done a lot of work using MRI-DTI (as well as PET). Dr. Wu can be contacted here.
Nuclear Medicine Imaging
Nuclear medicine imaging is not currently being used to assess individuals with possible DAI, however, iodine-123 single-photo emission (PET Scan) studies have demonstrated abnormal brain function in areas that MRI studies have missed.
Laboratory Studies in Diffuse Axonal Injury
There are current no commerically available lab studies that aid in the diagnosis or treatment of Diffuse Axonal Injury, however, as understanding of the specific biochemical changes associated with axonal injury has progressed, it is hoped that eventually the biomarkers of DAI may be tested for in the bloodstream of accident victims in much the same way that we now measure troponin levels to diagnose acute MI (myocardial infarction). Please see the aforementioned paper by Douglas Smith M.D. et. al. for more on this.
Treatment of Diffuse Axonal Injury
Currently there are no known specific drug therapies to inhibit or reverse the process of nerve axon dysfunction in Diffuse Axonal Injury. As our understanding of the specific biochemical processes at work in DAI grows, especially in the early post-injury period, the development of chemical agents that target and arrest these changes will be a top priority of neuro-science. Along these lines, the paper by Douglas Smith M.D. et. al. looks at some of the possible future therapeutic approaches.
Drug therapy at this time is restricted to treating the neuropsychiatric and neurobehavioral conditions that may occur as a result of injury. Depression, anxiety, agitation, and impulsive behavior may respond to specific pharmacologic agents, but great care must be taken in the administration of such medications to DAI patients. Symptoms may be aggravated rather than reduced, and because the symptoms of Diffuse Axonal Injury often change over time (especially during the first few years after injury), long-term pyschotropic drug regimens without frequent reassessment and follow up are to be avoided.
Prognosis in Diffuse Axonal Injury
90% of individuals with severe DAI remain in a persistent vegetative state indefinitely, and may remain so for decades. Of the 10% who regain consciousness, the majority will sustain permanent and far-reaching functional deficits as reviewed above. Only a small percentage of these individuals will attain near-normal neurological function. What improvement occurs usually does so within the first 12-24 months after the injury, although a small percentage of individuals may experience improvement, or deterioration, in their condition after this time.
In general, if a patient suffering head injury with DAI has a Glasgow Coma Scale score of 8 or less in the immediate post-injury period, the chances of permanent and severe neurological dysfunction are very likely.
Simon Fleminger, M.D., in an article in the Psychiatric Times in 2010, stated that measurement of PTA can provide a useful guide to prognosis in patients with Diffuse Axonal Injury. “As a rule, if PTA lasts less than 1 week, a reasonably good outcome is expected. If PTA lasts longer than 1 month, significant disability is likely; a good proportion of those affected will not be able to return to work or to independent living.In general, younger individuals (those in their late teens or 20s) tend to do much better.
The outlook for those with mild or moderate Diffuse Axonal Injury is better, especially for teens and individuals in their 20s.
Cal Shipley, M.D. copyright 2020